Subjective
History
Ownership: 9 months (rescue).
Familial/pertinent history: –
Reason for physiotherapy referral: Pelvic limb ‘stiffness’ after rest. Intermittent, left hind (LH) lameness during exercise.
Coxofemoral, stifle and lumbar radiographs 31/07/23- moderate, bilateral coxofemoral osteoarthritis (OA). Conservative management advised.
Condition noticed: 15/06/23.
Condition status: Improving. Initially stiff for 20 minutes and 2-3 x weekly, 2/4 LH gait ~15 minutes into walk. Since 06/08/23, stiff for 10 minutes and 1-2 x weekly, 1/4 LH gait ~30 minutes into walk.
Medication/s: 04/08/23 Librela (q 4 weeks).
Supplements: Antinol.
Known allergies: –
Diet: Royal Canin Satiety 378g BID. Bowl (kitchen floor).
Current/previous rehabilitation: –
Behaviour
People: –
Animals: Avoids boisterous dogs (static).
Grooming: Sitting down more (last ~3 months).
Sounds: Vocalization during thunderstorms (static).
Sleep: Night pacing/panting (improving last 2 weeks).
Toileting: Cocking hindlegs again (last 2 weeks).
Play: –
Motivational drivers: Food, chasing ball.
Home Environment
Flooring: Laminate. (Upstairs carpeted).
Furniture access: Settee.
Garden access: Small step (~50cm).
Stairs: Choosing not to go upstairs (last 2 months). ‘Bunny hops’ steps.
Car: Jumps in/out.
Bed and position: Settee. Choosing to sleep in the hall (last 2 months).
Exercise
Current exercise: 30 minutes BID woodland. Unlimited garden access. ~10 minutes/day catch.
On: off lead (%): 75: 25
Previous exercise: 1 hour off lead walk BID road/woodland. ~ a 2 hour walk on Saturdays. ~20 minutes/day catch.
Additional Information
Owner’s expectations: Pain free. Enjoy longer walks.
LOAD Score: 28 (severe).
Objective
Static
Demeanor: Bright, alert.
Body condition score (WSAVA): 7
Lateral: Occasionally toe touching LH.
Cranial Aspect: Cranially loading. Mild, bilateral elbow abduction.
Caudal Aspect: Low tail carriage. Narrow based hindleg (HL) stance- bilateral hock adduction.
Dorsal Aspect: Moderate, lumbar kyphosis.
Force plate: –
Dynamic
Surface type / restraint: Flat, concrete. Ruffwear harness and lead (walked on right).
Walk score: 1 (LH) Trot score: not performed due to walk score.
Score:
0= no lameness
1= mild lameness
2= obvious lameness with partial weight bearing
3= obvious lameness with intermittent weight bearing
4= non-weight bearing lameness
Description:
-Intermittently pacing.
-Pronounced pelvic sway (↑ movement R).
-Moderate L hip hike and delay initiating LH flexion in swing phase.
-Tail carriage low and fixed.
-Occasional HL ‘bunny hop’.
-Bilateral HL medial circumduction (LH > RH).
-Occasional, audible HL scuff.
Neurological Assessment
Not required.
Functional Movement
Spinal ROM: L lateral neck bend ↑ vs R (R: mid thorax / L: shoulder).
Sit/lie to stand: Labored (~15 seconds) initiates movement with forelimbs.
Stand to sit/lie: Labored (~10 seconds / multiple requests). HL bilateral stifle abduction, LH>RH.
Lead walking over 6 ground poles (30 cm apart): Knocks 1-2 poles LH (4/5 attempts).
Circling clockwise/ anticlockwise: LH stride length decreased anticlockwise.
Walking on uneven surfaces: Reluctant to walk on mattress.
Standing with FL on 10 cm step: 20 seconds, weight shifting LH exaggerated.
Steps: Bunny hop over single step.
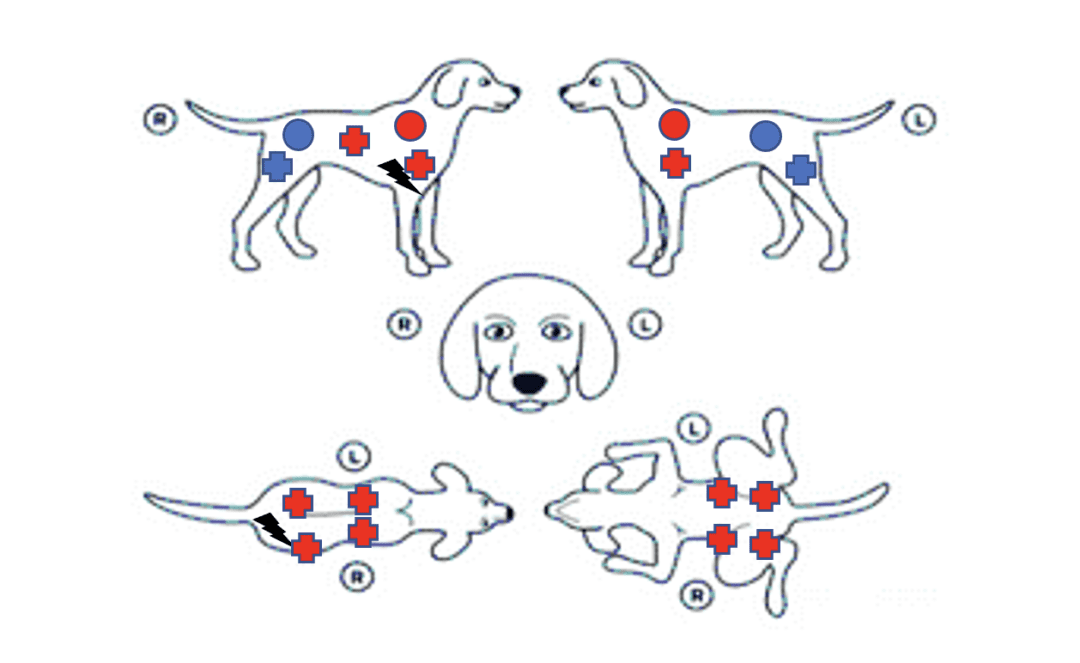
Palpation
Key:

-Marked hypertonicity: R>L lumbar paraspinals, L>R iliopsoas and L>R gracilis.
-Marked hypertonicity and hypertrophy: thoracic trapezius (R>L),
-Moderate hypotonicity and hypotrophy: gluteal, hamstrings (L>R).
-TRP: mid R long head of triceps (++fasciculations), R mid lumbar paraspinals.
– Reaction (lip licking): hip extension (L>R).
Measurements
Limb circumference (cm): mid femur. RH 22 LH 21
| Hindlimb (normal range) | Right | Left |
| Hip (50° – 162°)Flexion ExtensionEnd FeelPosition: lateral recumbency | 55130Pain | 60 120+ Pain, restricted extension |
Assessment
Problems
- Reduced PROM bilateral hips (L>R) and pain L hip extension.
- Offloading LH.
- Hypertonicity L>R gracilis and iliopsoas and R lumbar paraspinals.
- Hypertonicity and hypertrophy bilateral trapezius (R>L).
- TRP R long head of triceps and R lumbar paraspinals.
- Obesity.
Treatment
- PMFT (triple concentric, constant/200 Hz): 45 minutes- placed underneath patient (lying in lateral recumbency) during treatment.
- Thermotherapy (wheat pack, microwave 2 mins): lumbar and shoulders (3 mins each).
- Effleurage, myofascial release, R shoulder extension stretch (15 seconds): R long head triceps.
- Effleurage, ischemic compressions: R lumbar paraspinals.
- Effleurage, petrissage, Class 3 laser therapy (3.7J/cm2): bilateral gracilis and iliopsoas.
- Tapotement: bilateral gluteal and hamstrings.
- Class 3 laser (3.7J/cm2): bilateral, lateral hips.
- PROM bilateral hips, 10 repetitions.
- Grade 2 Maitland’s mobilization, extension stretch (15 seconds): bilateral hips.
- Weight shift: front feet on 10 cm step and lateral neck ROM (to shoulder) x 3 repetitions, hold for 5 seconds (TID).
Comment
Tolerated well. ↑ ROM L coxofemoral joint 2 degrees. ↓ Hypertonicity of R triceps/ R lumbar paraspinals with kyphosis improvement.
Goals (Objective Markers)
- Correct HL asymmetry (thigh measurements q 2 weeks).
- Improve gait and stance (palpation, static analysis weekly).
- Improve hip ROM (dynamic score, goniometer measurements and monitor functional movements weekly).
- Reduce LOAD and BCS (evaluate q 3 weeks).
- Improve fitness and monitor sleeping patterns (collar pedometer).
Treatment Schedule
Weekly (for 4 weeks).
Home Plan
Physiotherapeutic aims of canine coxofemoral osteoarthritis treatment are to relieve pain arising from the inflamed joint and secondary myofascial sources such as trigger points and hypertonicity, improve muscle strength, normalize gait patterns, regain, and maintain joint mobility and advise on lifestyle modifications (Millis and Levine, 1997). This essay is divided into sections critiquing the treatments selected according to the problem list in the preceding SOAP report.
Pain Relief
Cellular effects of pulsed magnetic field therapy (PMFT) include regulation of pro-inflammatory cytokines (Markov, 2020) and enhancement of neovascularization (Gaynor, 2018), making it useful in reducing inflammation in conditions such as osteoarthritis (Zhou et al., 2016). The author chose a treatment duration of 45 minutes as this provides the shortest beneficial application according to Watson (2021). Infrequent treatments (once only, or 2-3 times a week), appear less efficacious, so it may have been beneficial for the owner to attend sessions more regularly to attain maximum benefits of PMFT.
Laser therapy has been shown to decrease musculoskeletal pain (Haussler, 2020) however Edge-Hughes (2007) argues that effective penetration to the coxofemoral joint is questionable due to its structure. Another electrotherapy that could have been utilized is transcutaneous neuromuscular stimulation (TENS). TENS has been shown to be an effective adjunct alongside medication and exercise prescription in chronically painful conditions (Son et al., 2016) and can be used safely by owners as part of a home management plan (Cherian et al., 2016).
According to Plews-Ogan et al., (2005), massage stimulates the release of endorphins, activates neuropeptides, and provides pain relief if regular treatments are given. Therefore, instructing the owner on correct massage technique could enhance its analgesic effects.
Heat therapy was chosen over cryotherapy to provide local pain-relief as according to Oosterveld and Rasker (1994), it reduces nerve sensitivity and increases blood flow thereby causing muscle relaxation, and increased flexibility. In acute conditions, cryotherapy can reduce inflammation, and improve range of motion (Adie et al., 2012), however its efficacy in chronic conditions is yet to be established. The application of heat therapy to hypertonic regions could have been demonstrated to the owner to continue as part of the home treatment regime.
Manual Therapy
In human studies, manual therapy used in conjunction with exercise has a greater effect than exercise alone when treating coxofemoral osteoarthritis (Hoeksma et al., 2004). Osteoarthritic coxofemoral joints seemingly lose extension more than flexion (Johnston et al., 2008) therefore PROM was not only performed as an assessment tool but to provide sensory stimulation and prevent adaptive muscle shortening. Stretching and joint mobilizations were carried out as they facilitate synovial fluid flow which improves joint nutrition. The author chose to use grade 2 Maitland’s mobilization to have a neuro-modulatory effect on the coxofemoral joint (Lederman, 2005).
Exercise
Patients displaying discomfort from osteoarthritis should reduce daily activity (including play) until pain scores improve and gradually build up exercise to a tolerable level (Renberg, 2005), so the patient was advised to cease ball catching and walks over 15 minutes until assessment scores had improved. According to Weigl et al., (2004), low impact exercise involving isokinetic muscle strengthening (standing front feet on a raised platform) can significantly reduce pain associated with osteoarthritis. Once the patient is achieving therapeutic goals, more challenging exercises (sit-to-stands) could be introduced.
The benefits of underwater treadmill walking to improve aerobic conditioning and aid with weight loss have been described by Mlacknik et al., (2006). Owing to the patient’s body score and to improve gait pattern, it would have been beneficial to also discuss hydrotherapy referral with the owner.
40-80% of information given by medical practitioners is immediately forgotten by patients (Kessels, 2003) and with this in mind, the author felt it prudent not to overwhelm the owner with more than one therapeutic exercise.
References
Adie, S., Kwan, A., Naylor, J. M., Harris, I. A., & Mittal, R. (2012). Cryotherapy following total knee replacement. The Cochrane database of systematic reviews, (9), CD007911.
Canapp, S.O. (2007) ‘The Canine Stifle’, Clinical techniques in small animal practice, 22(4), pp. 195–205. doi: 10.1053/j.ctsap.2007.09.008.
Cherian, J. J., Harrison, P.E., Benjamin, S.A., Bhave, A., Harwin, S.F., & Mont, M. A. (2016). Do the effects of transcutaneous electrical nerve stimulation on knee osteoarthritis pain and function last? J Knee Surg, 29, 497-501.
Drum M. G. (2010). ‘Physical rehabilitation of the canine neurologic patient.’ The Veterinary clinics of North America. Small animal practice, 40(1), 181–193.
Edge-Hughes L. (2007). Hip and sacroiliac disease: selected disorders and their management with physical therapy. Clinical techniques in small animal practice, 22(4), 183–194.
Gaynor, J. S., Hagberg, S., & Gurfein, B. T. (2018). Veterinary applications of pulsed electromagnetic field therapy. Research in veterinary science, 119, 1–8.
Hoeksma, H. L., Dekker, J., Ronday, H. K., Heering, A., Van Der Lubbe, N., Vel, C., Breedveld, F. C., & Van Den Ende, C. H. . (2004). Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: A randomized clinical trial. Arthritis and Rheumatism, 51(5), 722–729.
Johnston, S., McLaughlin, R., & Budsberg, S. (2008). Nonsurgical Management of Osteoarthritis in Dogs. The Veterinary Clinics of North America. Small Animal Practice, 38(6), 1449-1470.
Kessels R. P. (2003). Patients’ memory for medical information. Journal of the Royal Society of Medicine, 96(5), 219–222.
Lederman E. The Science and Practice of Manual therapy. 2nd ed. Elsevier: London. (2005)
Markov, M., Ryaby, J., and Waldorff, E. I. (Eds). (2020). Pulsed Electromagnetic Fields for Clinical Applications. London/New York: CRC Press.
Millis, D. L., & Levine, D. (1997). The role of exercise and physical modalities in the treatment of osteoarthritis. The Veterinary clinics of North America. Small animal practice, 27(4), 913–930.
Millis, D. L., & Levine, D. (2014). Canine Rehabilitation and Physical Therapy. Saint Louis: Elsevier Health Sciences.
Mlacnik, E., Bockstahler, B., Müller, M., Tetrick, M. ., Nap, R. ., & Zentek, J. (2006). Effects of caloric restriction and a moderate or intense physiotherapy program for treatment of lameness in overweight dogs with osteoarthritis. Journal of the American Veterinary Medical Association, 229(11), 1756–1760.
Oosterveld FG, Rasker JJ. Effects of local heat and cold treatment on surface and articular temperature of arthritic knees. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 1994 Nov;37(11):1578-82.
Plews-Ogan, M., Owens, J. E., Goodman, M., Wolfe, P., & Schorling, J. (2005). A pilot study evaluating mindfulness-based stress reduction and massage for the management of chronic pain. Journal of general internal medicine, 20(12), 1136–1138.
Renberg, W. C. (2005). Pathophysiology and management of arthritis. The Veterinary Clinics of North America. Small Animal Practice, 35(5), 1073–1091.
Son, S. J., Kim, H., Seeley, M. K., Feland, J. B., Hopkins, J. T. (2016). ‘Effects of transcutaneous electrical nerve stimulation on quadriceps function in individuals with experimental knee pain’. Scand J Med Sci Sports, 26, 1080-1090.
Walton, M. B., Cowderoy, E., Lascelles, D., & Innes, J. F. (2013). Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PloS one, 8(3), e58125.
Watson, T (2021). Magnetic Field Therapy. Available at: http://www.electrotherapy.org/modality/magnetic-therapy. (Accessed 27 April 2023).
Weigl, M., Angst, F., Stucki, G., Lehmann, S., & Aeschlimann, A. (2004). Inpatient rehabilitation for hip or knee osteoarthritis: 2 year follow up study. Annals of Rheumatic Diseases, 63(4), 360–368.